Stabilized DHAA (DeHydroAscorbic Acid)
https://en.wikipedia.org/wiki/Dehydroascorbic_acid
Ascorbic Acid

 DeHydroAscorbic Acid
DeHydroAscorbic AcidDehydroascorbic acid (DHA) is an oxidized form of ascorbic acid (vitamin C). It is actively imported into the endoplasmic reticulum of cells via glucose transporters.[citation needed] It is trapped therein by reduction back to ascorbate by glutathione and other thiols.[1] The (free) chemical radical semidehydroascorbic acid (SDA) also belongs to the group of oxidized ascorbic acids.
Although a sodium-dependent transporter for vitamin C exists, it is present mainly in specialized cells, whereas the glucose transporters, the most notable being GLUT1, transport Vitamin C (in its oxidized form, DHA)[2] in most cells, where recycling back to ascorbate generates the necessary enzyme cofactor and intracellular antioxidant, (see Transport to mitochondria).
The structure shown here for DHA is the commonly shown textbook structure. This 1,2,3-tricarbonyl is too electrophilic to survive more than a few milliseconds in aqueous solution, however. The actual structure shown by spectroscopic studies is the result of rapid hemiacetal formation between the 6-OH and the 3-carbonyl groups. Hydration of the 2-carbonyl is also observed.[3] The lifetime of the stabilized species is commonly said to be about 6 minutes under biological conditions.[4] Destruction results from irreversible hydrolysis of the ester bond, with additional degradation reactions following.[5]
Crystallization of solutions of DHA gives a pentacyclic dimer structure of indefinite stability. Recycling of ascorbate via active transport of DHA into cells, followed by reduction and reuse, mitigates the inability of humans to synthesize it from glucose.[6]
Hydration equilibria of DHA - the hemiacetal structure (center) is the predominant one. (Water molecules are not actually involved in the first equilibrium, since it is an "internal" hemiacetalisation. Real hydration strictly occurs only in the middle carbonyl group)
Transport to mitochondria
Vitamin C accumulates in mitochondria, where most of the free radicals are produced, by entering as DHA through the glucose transporters, GLUT10. Ascorbic acid protects the mitochondrial genome and membrane.[2]
Transport to the brain
Vitamin C does not pass from the bloodstream into the brain, although the brain is one of the organs that have the greatest concentration of vitamin C. Instead, DHA is transported through the blood–brain barrier via GLUT1 transporters, and then converted back to ascorbate.[7]
Use
Dehydroascorbic acid has been used as a vitamin C dietary supplement.[8]
As a cosmetic ingredient, dehydroascorbic acid is used to enhance the appearance of the skin.[9] It may be used in a process for permanent waving of hair[10] and in a process for sunless tanning of skin.[11]
In a cell culture growth medium, dehydroascorbic acid has been used to assure the uptake of vitamin C into cell types that do not contain ascorbic acid transporters.[12]
As a pharmaceutical agent, some research has suggested that administration of dehydroascorbic acid may confer protection from neuronal injury following an ischemic stroke.[7] The literature contains many reports on the antiviral effects of vitamin C,[13] and one study suggests dehydroascorbic acid has stronger antiviral effects and a different mechanism of action than ascorbic acid.[14] Solutions in water containing ascorbic acid and copper ions and/or peroxide, resulting in rapid oxidation of ascorbic acid to dehydroascorbic acid, have been shown to possess powerful but short-lived antimicrobial, antifungal, and antiviral properties, and have been used to treat gingivitis, periodontal disease, and dental plaque.[15][16] A pharmaceutical product named Ascoxal is an example of such a solution used as a mouth rinse as an oral mucolytic and prophylactic agent against gingivitis.[16][17] Ascoxal solution has also been tested with positive results as a treatment for recurrent mucocutaneous herpes,[17] and as a mucolytic agent in acute and chronic pulmonary disease such as emphysema, bronchitis, and asthma by aerosol inhalation.[18]
http://www.recverin.com
Our name is pronounced "ree SEE ver in," we are manufacturers and sellers of advanced, science-based solutions of Vitamin C for topical and dietary use. ReCverin LLC is founded in the science of Vitamin C, with particular focus on the oxidized form called DHAA. We believe that the more you know about this science, the more you will appreciate the value of our products.
ReCverin LLC
944 E. 3300 S.
Salt Lake City, UT 84106
(801) 556-6424
ReCverin C contains 10% L-ascorbic acid as a stabilized solution in pure, vegetable glycerin. It provides the moisturizing, collagen-stimulating and antioxidant power of L-ascorbic acid in an ultra-pure, fragrance-free, moisturizing base with no harsh chemical preservatives. For firmer, smoother, more radiant-looking skin, apply daily before any other skincare product to the face, neck, hands, arms, and other exposed skin.
Stratum corneum (the dead outer layer of skin) poses a significant barrier to absorption of the common form of Vitamin C called L-ascorbic acid. Therefore L-ascorbic acid serums are most effective for persons who also practice some type of exfoliation (which refers to physical or chemical techniques for removing stratum corneum). Nevertheless, daily topical use of a high-strength serum like ReCverin C has been shown to increase the Vitamin C concentration in skin to higher levels than can be achieved by oral ingestion of Vitamin C, even in persons who don't exfoliate. The pH of an L-ascorbic acid serum has been shown to be a critical factor; absorption is much improved in serums with pH values of 3.0 or lower. ReCverin C™ is formulated at pH 2.7 for best absorption.
ReCverin C compares to many competing high-strength Vitamin C serums, with these important differences:
ReCverin C is extremely stable. It will easily retain greater than 95% of its stated L-ascorbic acid concentration for a year when stored at typical room temperatures, and it will remain crystal clear and colorless. With ReCverin C, you are free to ignore any concerns about stability and/or yellowing of your Vitamin C skin serum!
ReCverin C does not contain emulsifiers, detergents, preservatives, colorants or fragrances. Formulated in pure vegetable glycerin, it does not require any unnatural chemical agents that can contribute to skin sensitivity or other problems. Glycerin is the natural humectant found in sebum, the fluid that skin normally secretes onto its own surface. This water-soluble, skin-identical moisturizer has been used for centuries for its cosmetic effects in smoothing and moisturizing the skin, and also for its soothing, beneficial effects on rough, dry and irritated skin.
ReCverin C is economical. The two-ounce bottle contains 2 or 4 times more serum than a bottle of most competing products.
Please be aware that some people experience tingling or irritation after applying high-strength L-ascorbic acid solutions. For most people, if they experience them at all, these effects are mild, temporary, and completely tolerable. But those with very sensitive skin can have difficulty using high-strength L-ascorbic acid.
We highly recommend our premiere product ReCverin 50/50 for those with sensitive skin, for those who don't regularly exfoliate, and, in fact, for anyone who is seeking maximum absorption of Vitamin C.
ReCverin C™ Use and Storage Guidelines
Apply daily to the face, neck, arms, hands and other exposed skin. Avoid direct contact with eyes.
We suggest using 3-5 drops for the face, and a similar application rate for other, similar-sized skin areas.
Apply to clean skin before any other products, and massage in thoroughly.
ReCverin C can be used directly as supplied, or it may be mixed with water immediately before applying. We suggest applying to moist skin or mixing with a little water by placing a few drops of water and product in the palm and rubbing the hands together. Water combines with the humectant glycerin base to create a deep-penetrating moisturizer that absorbs quickly and gives a skin texture that many people prefer. Vary the proportions to the consistency you desire.
ReCverin C blends nicely with most lotions. You can mix a few drops with another lotion immediately before applying, or you can apply another lotion immediately after applying our serum.
Please keep in mind that ReCverin C is carefully formulated to stabilize Vitamin C. One of the secrets to its stability is that it contains no water. We recommend that you do not premix with water or lotions for later use.
Store at room temperature or below. For best results, use within 1 year.
A Special Note for Do-It-Yourselfers
Making do-it-yourself skin care products is a popular hobby. We respect and admire those who blend their own in that quest for the perfect, individualized composition of ingredients! Both ReCverin C and ReCverin 50/50 can be utilized as a starting base or component of the water-soluble fraction of your own formulas.
A particularly popular composition among DIYers contains Vitamin C, Vitamin E, and Ferulic Acid, commonly known as a "CEF Serum," and there are many different and varied recipes. To demonstrate how our products can be used by DIY folks, we have prepared a video that shows how an excellent and easy CEF Serum can be prepared featuring ReCverin C. This recipe focuses on maintaining a water-free composition to preserve the remarkable stability of the Vitamin C component as provided in ReCverin C.
References :
2016) Arterial Tortuosity Syndrome reveals function of dehydroascorbic acid in collagen and elastin synthesis: Implications for skin care
(2016) Genetic Variation in Human Vitamin C Transporter Genes in Common Complex Diseases
(2015) Vitamin C selectively kills KRAS and BRAF mutant colorectal cancer cells by targeting GAPDH
(2015) Genetic Variants in GLUT14 Gene Enhance Susceptibility to Inflammatory Bowel Disease
(2014) Vitamin C Deficiency – Part 3
(2014) The oxidized form of vitamin C, dehydroascorbic acid, regulates neuronal energy metabolism
(2014) Subcellular compartmentation of ascorbate and its variation in disease states
(2014) Role of GLUT1 in regulation of reactive oxygen species
(2013) Regulation of Vitamin C Homeostasis during Deficiency
(2011) High dietary fat and cholesterol exacerbates chronic vitamin C deficiency in guinea pigs
(2011) Ascorbic acid attenuates lipopolysaccharide-induced acute lung injury
(2010) Glucose transporter 10 and arterial tortuosity syndrome: The vitamin C connection
(2009) Vitamin C function in the brain: vital role of the ascorbate transporter SVCT2
(2008) Antiviral effects of ascorbic and dehydroascorbic acids in vitro
(2007) Vitamin C: Biosynthesis, recycling and degradation in mammals
(2004) Vitamin C Is a Kinase Inhibitor: Dehydroascorbic Acid Inhibits IκBα Kinase β
(2003) Recycling of Vitamin C by a Bystander Effect
(2002) Vitamin C Prevents DNA Mutation Induced by Oxidative Stress
(2000) Ascorbate oxidation is a prerequisite for its transport into rat liver microsomal vesicles
(1998) Absorption, transport, and disposition of ascorbic acid in humans
(1997) Glucose Transporter Isoforms GLUT1 and GLUT3 Transport Dehydroascorbic Acid
(1996) Gluconeogenesis from ascorbic acid: ascorbate recycling in isolated murine hepatocytes
(1994) Enzymic and non-enzymic antioxidants in epidermis and dermis of human skin
(1993) Ascorbic acid recycling in human neutrophils
(1956) Aging: A Theory Based on Free Radical and Radiation Chemistry--by Denham Harman
(1944) Water Soluble Vitamins in Sweat
(1937) The Oxidation of Ascorbic Acid and its Reduction In Vitro and In Vivo
(1936) Vitamin C in Vegetables: Ascorbic Acid Oxidase
(1934) The urinary excretion of ascorbic and dehydroascorbic acids in man
https://www.youtube.com/watch?v=YHKBhz7OCB4
The discoverer claims it surpasses absorption limits of other forms of vitamin C and sites a number of studies so indicating.
There are different types of ports on the cells in the body, and one of the ports is for vitamin C.
The form of vitamin C disclosed in the video and on the web site is absorbed through the glucose ports on the cells, and there are 4-5 times more glucose ports than ascorbic acid/vitamin C ports in the cells, so much higher absorption rates are achieved with this form (it also takes energy to absorb vitamin C through the vitamin C ports, but it doesn't take energy to absorb through the glucose ports). (Absorption into blood stream from digestive tract and from blood stream into cells in the body). The cells can then convert this form of vitamin C back to the common form.

Scientific journal articles referenced in this video:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3065766/
Advances in Nutrition, 2(2):78-88 (2011)
Levine, M., S.J. Padayatty, and M.G. Espey
Abstract
A concentration-function approach to vitamin C (ascorbate) has yielded new physiology and pharmacology discoveries. To determine the range of vitamin C concentrations possible in humans, pharmacokinetics studies were conducted. They showed that when vitamin C is ingested by mouth, plasma and tissue concentrations are tightly controlled by at least 3 mechanisms in healthy humans: absorption, tissue accumulation, and renal reabsorption. A 4th mechanism, rate of utilization, may be important in disease. With ingested amounts found in foods, vitamin C plasma concentrations do not exceed 100 μmol/L. Even with supplementation approaching maximally tolerated doses, ascorbate plasma concentrations are always <250 μmol/L and frequently <150 μmol/L. By contrast, when ascorbate is i.v. injected, tight control is bypassed until excess ascorbate is eliminated by glomerular filtration and renal excretion. With i.v. infusion, pharmacologic ascorbate concentrations of 25–30 mmol/L are safely achieved. Pharmacologic ascorbate can act as a pro-drug for hydrogen peroxide (H2O2) formation, which can lead to extracellular fluid at concentrations as high as 200 μmol/L. Pharmacologic ascorbate can elicit cytotoxicity toward cancer cells
and slow the growth of tumors in experimental murine models. The effects of pharmacologic ascorbate should be further studied in diseases, such as cancer and infections, which may respond to generation of reactive oxygen species via H2O2...
Conclusions
A concentration-function approach to vitamin C yields new insights into its physiology and pharmacology. Vitamin C concentrations are tightly controlled with oral ingestion by at least 4 mechanisms. Disruption of one mechanism, renal reabsorption, reveals a new potential role of ascorbate in perinatal health and unanticipated feedback regulation of ascorbate biosynthesis. For proper clinical translation, dose concentration relationships must be accounted for in clinical studies. Tight control of ascorbate concentrations is bypassed with i.v. administration until renal excretion restores homeostasis. With i.v. administration, ascorbate is turned from vitamin to drug, as pharmacologic concentrations are produced that are as much as 100-fold higher than those possible with maximal oral dosing. Pharmacologic ascorbate, by acting as a pro-drug for H2O2 in the extracellular fluid, has potential in treatment of cancer, infectious diseases, and perhaps other conditions in which H2O2 may have efficacy. Ascorbate administered intravenously has already been tested in a phase I clinical trial, is in wide use by complementary and alternative medicine (integrative medicine) practitioners, and appears to have minimal side effects in patients who are properly screened.
http://69.164.208.4/files/Pharmacokinetics%20of%20oral%20vitamin%20C.pdf
Journal of Nutritional & Environmental Medicine 17(3): p. 169-177 (2008)
Hickey, S., H.J. Roberts, and N.J. Miller.
https://www.youtube.com/watch?v=cwwdk9scG64&feature=youtu.be
See how to make an economical, effective and elegant skin serum with vitamin C, vitamin E, and ferulic acid.
Ingredients:
1 bottle ReCverin C TM or ReCverin 50/50 TM from www.ReCverin.com
1/8 tsp ferulic acid
18 drops vitamin E oil
18 drops polysorbate 80
(from a supplier of ingredients for DIY skin care like Lotioncrafter or Skin Essentials Actives)
https://www.researchgate.net/publication/225274699_Topical_Dehydroascorbic_Acid_Oxidized_Vitamin_C_Permeates_Stratum_Corneum_More_Rapidly_Than_Ascorbic_Acid?ev=prf_pub_p2
Abstract
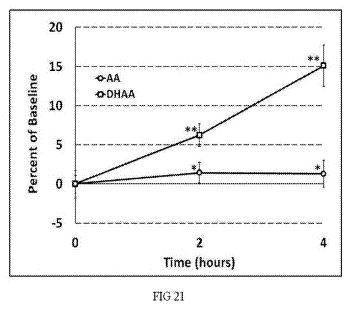
Topical application of vitamin C has an established history of use in skincare. A large body of literature from clinical and laboratory studies supports a scientific basis for its use in improving both the appearance and health of the skin. Ascorbic acid (AA) is the naturally-occurring chemical form of vitamin C that is most familiar, and it is commonly used in topical products. But AA has limited permeation through the stratum corneum, and this has led to the use of very high concentrations that are associated with side effects such as tingling, irritation and redness in some people. Dehydroascorbic acid (DHAA) is the other naturally-occurring form of vitamin C, and has chemical properties that suggest its skin permeation rate would be higher than AA. In this study, the rates of AA and DHAA permeation were compared by a clinically relevant, in vivo method on human subjects. Specifically, a solution containing equal parts of AA and DHAA was applied in amounts and for time periods likely to be achieved in common use of a topical product by consumers. The amount absorbed was determined by subtracting the amount recoverable in skin washings. The results show that DHAA permeates stratum corneum at a rate up to 12 times faster than AA. This supports the concept that lower concentrations of DHAA in topical preparations can enhance skin vitamin C levels with less potential for side effects…
DHAA is a more lipophilic compound than AA, and it is not ionized in aqueous solution [11]. Both of these properties suggest that DHAA would permeate the stratum corneum more easily [12]. The aim of the present study was to compare the rate of AA versus DHAA absorption in order to assess whether or not DHAA actually does permeate more easily. A solution containing both AA and DHAA in approximately equal concentrations was used to compare their absorption rates in vivo, using a simple, non-invasive technique on human subjects. To assess permeation into the stratum corneum, the solution was applied to delineated skin surfaces and allowed 0, 2 or 4 hours for absorption. Each skin surface was then washed with deionized water, and the skin washings were collected and measured for AA and DHAA content. The amount absorbed at 2 and 4 hours was determined by subtraction from the amount present in the 0 hour washings. The aim of the study was achieved, since measurable differences in AA versus DHAA absorption were observed, and the DHAA absorption rate was found to be significantly greater than that of AA…

http://www.sciencedirect.com/science/article/pii/S2213231715300045
doi:10.1016/j.redox.2015.11.003
Redox Biology, Volume 7, April 2016, Pages 8–13
Henriette Frikke-Schmidt, Pernille Tveden-Nyborg, Jens Lykkesfeldt,
Highlights
Dehydroascorbic acid is an effective vitamin C source in guinea pigs.
Like in humans, efficient recycling of vitamin C has evolved in guinea pigs.
The guinea pig is a better model of human vitamin C homeostasis than rat and mouse.
Abstract
Vitamin C deficiency globally affects several hundred million people and has been associated with increased morbidity and mortality in numerous studies. In this study, bioavailability of the oxidized form of vitamin C (l-dehydroascorbic acid or DHA)—commonly found in vitamin C containing food products prone to oxidation—was studied. Our aim was to compare tissue accumulation of vitamin C in guinea pigs receiving different oral doses of either ascorbate or DHA. In all tissues tested (plasma, liver, spleen, lung, adrenal glands, kidney, muscle, heart, and brain), only sporadic differences in vitamin C accumulation from ascorbate or DHA were observed except for the lowest dose of DHA (0.25 mg/ml in the drinking water), where approximately half of the tissues had slightly yet significantly less vitamin C accumulation than from the ascorbate source. As these results contradicted data from rats, we continued to explore the ability to recycle DHA in blood, liver and intestine in guinea pigs, rats and mice. These investigations revealed that guinea pigs have similar recycling capacity in red blood cells as observed in humans, while rats and mice do not have near the same ability to reduce DHA in erythrocytes. In liver and intestinal homogenates, guinea pigs also showed a significantly higher ability to recycle DHA compared to rats and mice. These data demonstrate that DHA in guinea pigs—as in humans—is almost as effective as ascorbate as vitamin C source when it comes to taking up and storing vitamin C and further suggest that the guinea pig is superior to other rodents in modeling human vitamin C homeostasis.
Exp Neurobiol. 2015 Mar;24(1):41-54. English.
http://dx.doi.org/10.5607/en.2015.24.1.41
Juhyun Song, Joohyun Park, Jae Hwan Kim, Ja Yong Choi, Jae Young Kim, Kyoung Min Lee, and Jong Eun Lee
Abstract
Ischemic stroke results in the diverse phathophysiologies including blood brain barrier (BBB) disruption, brain edema, neuronal cell death, and synaptic loss in brain. Vitamin C has known as the potent anti-oxidant having multiple functions in various organs, as well as in brain. Dehydroascorbic acid (DHA) as the oxidized form of ascorbic acid (AA) acts as a cellular protector against oxidative stress and easily enters into the brain compared to AA. To determine the role of DHA on edema formation, neuronal cell death, and synaptic dysfunction following cerebral ischemia, we investigated the infarct size of ischemic brain tissue and measured the expression of aquaporin 1 (AQP-1) as the water channel protein. We also examined the expression of claudin 5 for confirming the BBB breakdown, and the expression of bcl 2 associated X protein (Bax), caspase-3, inducible nitric oxide synthase (iNOS) for checking the effect of DHA on the neurotoxicity. Finally, we examined postsynaptic density protein-95 (PSD-95) expression to confirm the effect of DHA on synaptic dysfunction following ischemic stroke. Based on our findings, we propose that DHA might alleviate the pathogenesis of ischemic brain injury by attenuating edema, neuronal loss, and by improving synaptic connection.
INTRODUCTION
Ischemic stroke is the second leading cause of death worldwide accompanied by severe disability [1]. Cerebral ischemia and reperfusion injury leads to damage of brain tissues, inflammation as a result of the blood-brain barrier (BBB) disruption, oxidative damage [2], and apoptosis [3]. Brain tissue is highly vulnerable to oxidative damage because of its high use of oxygen [4] under cerebral ischemia. Cerebral ischemia leads to loss of tight junction proteins in brain endothelium, BBB disruption, and finally brain edema [5]. Brain edema leads to an imbalance in energy demand and influences on the postsynaptic effects of glutamate [6] and interruption of synaptic transmission in the penumbra after stroke [7, 8]. Overall, excitotoxicity, inflammation and oxidative stress caused by ischemic stroke plays a crucial role in the pathophysiology of ischemic stroke [9, 10]. To reduce the brain damage caused by cerebral ischemia, the solution for oxidative damage is the issue of the greatest importance. Vitamin C is the most important antioxidant for metabolic function of the brain [11, 12, 13] owing to its low redox potential which is capable of neutralizing diverse pro oxidants [14, 15, 16, 17]. Mainly, vitamin C could be found in its form such as ascorbic acid (AA) and dehydroascorbic acid (DHA) (AA's oxidized form) [18, 19]. According to earlier studies, lower levels of vitamin C are a risk factor of cerebral stroke [20, 21] and actually, decreased vitamin C levels has been demonstrated in patients with ischemic stroke [22]. Recent study demonstrated that the treatment of AA prevented the disruption of BBB and sustained the BBB integrity in the cortex [23]. Neuroprotection by DHA has been demonstrated in several recent studies in both in vitro and in vivo. In in vitro study, DHA has been reported that it inhibits mitochondrial damage and cell death against oxidative injury [24]. Specifically, DHA among vitamin C could crosses the BBB through glucose transporter 1 (GLUT1) [25] and prevents cell death against oxidative damage by increasing glutathione (GSH) levels through glucose transporters [26, 27]. In in vivo study, DHA have been reported to have protective effects as antioxidants in experimental neurological disease models such as stroke [19, 28, 29, 30]. DHA administration attenuates oxidative stress markers and inflammation in hyperglycemic stroke models [31]. However, the study on the role of DHA administration through intra-peritoneal route in ischemic stroke animal model focused on edema formation, neurotoxicity, and synaptic dysfunction has not yet been determined. In present study, we investigated DHA's beneficial effect after ischemic brain injury in in vivo study. Our results show that DHA is involved in the prevention of brain edema formation, neurotoxicity, and synaptic dysfunction following ischemia injury. Thus, we suggest that DHA might mitigate stroke-induced pathological alterations following cerebral ischemic stroke...
RESULTS
DHA reduced brain edema formation following cerebral ischemia
...The percentage of brain edema in the MCAO group was >12% whereas the percentage of brain edema after DHA treatment was <8% (Fig. 1C). Brain edema (%) was significantly reduced in the DHA group compared with the MCAO group. Our results indicate that the DHA treatment reduced brain edema formation after ischemic brain injury...
DHA reduced the expression of AQP-1 as the marker of vascular permeability following cerebral ischemia...
DHA attenuates the cell damage against neurotoxicity following cerebral ischemia…
DHA prevents the damage of post synaptic plasticity following cerebral ischemia…
DISCUSSION
Ischemic stroke causes the blockage of cerebral blood vessels in the regions of brain, which can lead to human disability and death [36]. Subsequently, the blockage of blood vessels following stroke leads to diverse pathophysiologies including brain edema, neuronal loss, and cognitive dysfunction [37, 38, 39, 40]. Cerebral cortex, hippocampus, and corpus striatum in the brain are the most vulnerable regions against oxidative stress and hypoxic injury induced by cerebral ischemia [41]. Many studies has reported that vitamin C among antioxidants is generally neuroprotective in response to brain ischemic injury [42, 43, 44, 45]. Oral administration of AA to animal had demonstrated that it suppresses neuronal damage under cerebral ischemia-reperfusion [46]. Dehydroascorbic acid as AA's oxidized form [15, 18, 19] has been reported that it has a neuroprotective role [47] and is easily transported to the brain by mediating glucose transporter 1 (GLUT1) located in the endothelial cells of the BBB [48]. However, DHA did not fully be investigated in ischemic stroke animal model in spite of its advantages. We anticipated that DHA as an anti-oxidant may considerably affect on cerebral ischemia animal because it can rapidly pass through the brain than AA [25]. In present study, we investigated the neuroprotective effects of brain by DHA i.p administration in cerebral ischemia rat. First, we obtained the consequence that DHA treatment inhibits the brain edema formation in MCAO rat brain. Edema defined as an abnormal increase in brain water content is frequently observed in cerebral ischemia and also has a critical influence on morbidity and mortality [49]. Several studies reported that cerebral ischemia contributes to damage the integrity and permeability of the BBB [50, 51]. Aquaporin (AQP) is the water channel protein that facilitates water transport through cell membranes [52, 53]. Specifically AQP-1 is permeable only to water and is considered to participate in brain water homeostasis [54]. In addition, AQP 1 has been reported that it is involved in edema formation and cell death in the hippocampus following brain injury [55]. Following our results, we suggest that DHA may reduce osmotic water permeability following cerebral ischemia by inhibiting the expression of AQP-1. All BBB components have been reported to the association with the regulation of the BBB permeability including tight junctions of endothelial cells, glia cells [56, 57, 58]. The BBB is composed of the brain endothelial cells interconnected with transmembrane tight junction proteins such as claudin-5 [59] and regulates paracellular permeability [60, 61]. In present study, our results indicated that claudin 5 as a tight junction protein in DHA treated MCAO rat brain was evidently preserved against ischemic injury. According to our results, DHA may protect the BBB integrity by preserving tight junction protein in response to ischemic injury. Cerebral ischemia induces the neurotoxic environment in brain and it could result in the severe neuronal cell damage, so we investigated the cell death marker such as Bax [62, 63], caspase-3[64, 65], and iNOS [66, 67] in order to examine the protective effect of DHA against the neurotoxicity following ischemic stroke. In present study, DHA treatment reduced the expression of Bax and caspase-3 which is the marker of the mitochondrial cell death and iNOS in ischemic injured brain. Nitric oxide (NO) that causes neuronal cell death and exacerbates glutamate toxicity after cerebral ischemia [68] is synthesized by NO synthase such as iNOS [69]. Several studies demonstrated that inhibition of iNOS in cerebral ischemia improves neurological deficits and reduces infarct volume [70, 71]. In consideration of Figure 1 result, our finding suggested that DHA attenuates the expression of iNOS and it may be linked to reduced infarct volume and improved cell death against hypoxic injury. Additionally, NO formed by iNOS has been reported the implicated in neurodegeneration [69]. Judging from our result regarding the reduced iNOS expression, we suggest the possibility of DHA regarding the improvement of cognitive function against ischemic stroke although we did not check the production of NO and behavior test considering that AA improves the cognitive decline in Alzheimer's disease [72]. As mentioned earlier, several studies demonstrated that DHA prevents cell death against ischemic injury [19, 28, 29, 30]. However, previous studies have not yet been determined the effect of DHA on recovery of neuronal function in ischemia animal model. Therefore, we tried to examine the effect of DHA on neuronal function by measuring indirectly synaptic dysfunction in present study. In order to observe the effect of DHA on ischemia-induced synaptic connection alteration, we investigated the expression of PSD-95 protein in ischemic brain tissue. PSD-95 protein as a postsynaptic marker [73, 74] is a member of the membrane-associated guanylate kinase family of synaptic molecules and is localized at excitatory synapses [75]. Postsynaptic densities (PSD) proteins are involved in regulation of synaptic function and in the transduction of synaptic signals to the postsynaptic cell [76, 77, 78]. Especially, PSD-95 has been implicated in the regulation of ion-channel function, synaptic activity, and intracellular signaling and finally cognitive impairment [79, 80, 81]. In addition, PSD-95 protein is implicated in promoting synapse stability and makes synaptic contacts more stable in neurons [75]. Recent studies suggested that the PSD-95 protein improves the neurophysiologic phenomenon after ischemic stroke involving MCAO [82, 83]. Moreover, some researchers demonstrated that the decrease of PSD-95 protein immunoreactivity in the ischemic brain leads to a deficit of postsynaptic plasticity in the brain [84]. Several studies suggest that PSD-95's reduction is associated with cognitive impairment [85, 86, 87, 88]. Based on our results, our findings indicate that DHA induced the increase of PSD-95 protein immunoreactivity in ischemic stroke brain and DHA may improve the ischemic-induced synaptic plasticity dysfunction. In addition, although we did not check the memory function related behavior test such as water maze, we carefully expect that DHA may improve the learning and memory dysfunction following cerebral ischemia by promoting the neuron's synapse stability. Taken together, our findings suggest three points that 1) DHA is involved in the inhibition of AQP-1 expression and the preservation of claudin 5, ultimately resulting in the reduction of edema formation induced by cerebral ischemia, 2) DHA is associated with the decrease of Bax, cleaved caspase-3 and iNOS expression, ultimately resulting in the protection of cell death against neurotoxicity following cerebral ischemia, 3) DHA is linked to the preservation of PSD-95 protein expression, ultimately resulting in the improvement of neuron's synaptic connection in cerebral ischemia. The present study has some limitations fully to prove the beneficial effect of DHA against ischemic injury. However, we suggest that this study is worthy in that it provide the need of the further study of DHA on ischemic stroke. Taken together, we propose that the DHA might be beneficial to alleviate clinical pathologies that occur after ischemic stroke.
http://www.ncbi.nlm.nih.gov/pubmed/24460956
J Neurochem. 2014 May;129(4):663-71.
doi: 10.1111/jnc.12663. Epub 2014 Feb 19.
Cisternas P, Silva-Alvarez C, Martínez F, Fernandez E, Ferrada L, Oyarce K, Salazar K, Bolaños JP, Nualart F.
Abstract
Vitamin C is an essential factor for neuronal function and survival, existing in two redox states, ascorbic acid (AA), and its oxidized form, dehydroascorbic acid (DHA). Here, we show uptake of both AA and DHA by primary cultures of rat brain cortical neurons. Moreover, we show that most intracellular AA was rapidly oxidized to DHA. Intracellular DHA induced a rapid and dramatic decrease in reduced glutathione that was immediately followed by a spontaneous recovery. This transient decrease in glutathione oxidation was preceded by an increase in the rate of glucose oxidation through the pentose phosphate pathway (PPP), and a concomitant decrease in glucose oxidation through glycolysis. DHA stimulated the activity of glucose-6-phosphate dehydrogenase, the rate-limiting enzyme of the PPP. Furthermore, we found that DHA stimulated the rate of lactate uptake by neurons in a time- and dose-dependent manner. Thus, DHA is a novel modulator of neuronal energy metabolism by facilitating the utilization of glucose through the PPP for antioxidant purposes.
http://www.jbc.org/content/288/13/9092.full
Christopher P. Corpe, Peter Eck, Jin Wang, Hadi Al-Hasani and Mark Levine
Background: The molecular identity of the intestinal vitamin C transporters is incomplete.
Results: Facilitative sugar transporters, GLUT2 and GLUT8, transport dehydroascorbic acid, the oxidized form of vitamin C.
Conclusion: Intestinal vitamin C absorption can occur via facilitative sugar transporters.
Significance: Vitamin C bioavailability may be inhibited by dietary factors, such as glucose and phytochemicals.
Abstract
Intestinal vitamin C (Asc) absorption was believed to be mediated by the Na+-dependent ascorbic acid transporter SVCT1. However, Asc transport across the intestines of SVCT1 knock-out mice is normal indicating that alternative ascorbic acid transport mechanisms exist. To investigate these mechanisms, rodents were gavaged with Asc or its oxidized form dehydroascorbic acid (DHA), and plasma Asc concentrations were measured. Asc concentrations doubled following DHA but not Asc gavage. We hypothesized that the transporters responsible were facilitated glucose transporters (GLUTs). Using Xenopus oocyte expression, we investigated whether facilitative glucose transporters GLUT2 and GLUT5–12 transported DHA. Only GLUT2 and GLUT8, known to be expressed in intestines, transported DHA with apparent transport affinities (Km) of 2.33 and 3.23 mm and maximal transport rates (Vmax) of 25.9 and 10.1 pmol/min/oocyte, respectively. Maximal rates for DHA transport mediated by GLUT2 and GLUT8 in oocytes were lower than maximal rates for 2-deoxy-d-glucose (Vmax of 224 and 32 pmol/min/oocyte for GLUT2 and GLUT8, respectively) and fructose (Vmax of 406 and 116 pmol/min/oocyte for GLUT2 and GLUT8, respectively). These findings may be explained by differences in the exofacial binding of substrates, as shown by inhibition studies with ethylidine glucose. DHA transport activity in GLUT2- and GLUT8-expressing oocytes was inhibited by glucose, fructose, and by the flavonoids phloretin and quercetin. These studies indicate intestinal DHA transport may be mediated by the facilitative sugar transporters GLUT2 and GLUT8. Furthermore, dietary sugars and flavonoids in fruits and vegetables may modulate Asc bioavailability via inhibition of small intestinal GLUT2 and GLUT8.
http://www.ingentaconnect.com/content/sp/ijmm/2008/00000022/00000004/art00018
International Journal of Molecular Medicine, Volume 22, Number 4, 2008, pp. 541-545(5)
http://dx.doi.org/10.3892/ijmm_00000053
Furuya, Ayami; Uozaki, Misao; Yamasaki, Hisashi; Arakawa, Tsutomu; Arita, Mikio; Koyama, A. Hajime
Abstract:
In the present study, ascorbic acid weakly inhibited the multiplication of viruses of three different families: herpes simplex virus type 1 (HSV-1), influenza virus type A and poliovirus type 1. Dehydroascorbic acid, an oxidized form of ascorbic acid and hence without reducing ability, showed much stronger antiviral activity than ascorbic acid, indicating that the antiviral activity of ascorbic acid is due to factors other than an antioxidant mechanism. Moreover, addition of 1 mM Fe3+, which oxidizes ascorbic acid to dehydroascorbic acid and also enhances the formation of hydroxyl radicals by ascorbic acid in the culture media, strongly enhanced the antiviral activity of ascorbic acid to a level significantly stronger than that of dehydroascorbic acid. Although both ascorbic acid and dehydroascorbic acid showed some cytotoxicity, the degree of cytotoxicity of the former was 10-fold higher than the latter, suggesting that the observed antiviral activity of ascorbic acid with and without ferric ion is, at least in part, a secondary result of the cytotoxic effect of the reagent, most likely due to the free radicals. However, the possibility that oxidation of ascorbic acid also contributed to the antiviral effects of ascorbic acid exists, in particular in the presence of ferric ion, since dehydroascorbic acid exhibited a very strong antiviral activity. Characterization of the mode of antiviral action of dehydroascorbic acid revealed that the addition of the reagent even at 11 h post infection almost completely inhibited the formation of progeny infectious virus in the infected cells, indicating that the reagent inhibits HSV-1 multiplication probably at the assembly process of progeny virus particles after the completion of viral DNA replication.
http://onlinelibrary.wiley.com/doi/10.1002/art.21254/full
Arthritis & Rheumatism, Volume 52, Issue 9, pages 2676–2685, September 2005
DOI: 10.1002/art.21254
Amy L. McNulty, Thomas V. Stabler, Thomas P. Vail, Gary E. McDaniel and Virginia B. Kraus*
Abstract
Objective
To evaluate the dehydroascorbate (DHA) transport mechanisms in human chondrocytes.
Methods
The transport of L-14C-DHA in human chondrocytes was analyzed under various conditions, including the use of RNA interference (RNAi), to determine the role of glucose transporter 1 (GLUT-1) and GLUT-3 in L-14C-DHA transport and to evaluate the effects of physiologically relevant oxygen tensions on L-14C-DHA transport. In order to estimate the contributions of reduced ascorbic acid (AA) and DHA to intracellular ascorbic acid (Asc), the quantities of AA and DHA were measured in synovial fluid samples from osteoarthritis (OA) patients and compared with the reported levels in rheumatoid arthritis (RA) patients.
Results
DHA transport in human chondrocytes was glucose-sensitive, temperature-dependent, cytochalasin B–inhibitable, modestly stereoselective for L-DHA, and up-regulated by low oxygen tension. Based on the RNAi results, GLUT-1 mediated, at least in part, the uptake of DHA, whereas GLUT-3 had a minimal effect on DHA transport. DHA constituted a mean 8% of the total Asc in the synovial fluid of OA joints, in contrast to 80% of the reported total Asc in RA joints.
Conclusion
We provide the first evidence that chondrocytes transport DHA via the GLUTs and that this transport mechanism is modestly selective for L-DHA. In the setting of up-regulated DHA transport at low oxygen tensions, DHA would contribute 26% of the total intracellular Asc in OA chondrocytes and 94% of that in RA chondrocytes. These results demonstrate that DHA is a physiologically relevant source of Asc for chondrocytes, particularly in the setting of an inflammatory arthritis, such as RA.
Dehydroascorbic Acid Process
Processes to produce dehydroascorbic acid at the time of use are provided, so that this unstable form of vitamin C can be conveniently utilized for dietary purposes. Products produced by these processes are also described.
BACKGROUND
[0001] 1. Field of Invention
[0002] This invention relates to the field of improved absorption of orally ingested vitamin C, and more specifically to the form of vitamin C known as dehydroascorbic acid (DHAA). DHAA is the naturally-occurring oxidized form of vitamin C, and has many unique properties as compared to the reduced form, ascorbic acid (AA). Many of these properties are described in U.S. Pat. No. 8,324,269 which is incorporated herein in its entirety by reference.
[0003] Absorption of orally ingested vitamin C into the cells of the gut is mediated by transport proteins in the cell membrane. AA or ascorbate ion absorption occurs via various members of the family of transport proteins known as SVCT, whereas DHAA is absorbed utilizing members of the GLUT family. GLUT transporters are a type known as passive transporters, which in general means that they transport more rapidly than the type known as active transporters.
Also passive transport is not a saturable mechanism as is active transport. Furthermore, GLUT transporters are abundant in the nutrient-absorbing cells lining the gut because these transporters also transport common sugars like glucose. Taken together, these facts mean that DHAA can be absorbed much more rapidly and efficiently when orally ingested than can the more common AA, because the SVCT transport proteins are active transporters that can be saturated and are less abundant in the gut. Therefore oral consumption of DHAA has great advantages as compared to the oral consumption of AA that is found in common vitamin C supplements, including greater bioavailability of larger doses, more rapid absorption, and higher vitamin C blood levels post consumption.
[0004] 2. Prior Art
[0005] Background art includes U.S. patent application Ser. No. 10/572,790 (Mar. 21, 2006) of Gassier (now abandoned). Gassier describes a method of producing DHAA by supplying multi-part components that can be combined to cause the oxidation of ascorbate to DHAA for a cosmetic purpose. But Cassier's invention requires at least one cosmetic ingredient, and is silent as to the use of the product for oral ingestion.
SUMMARY OF INVENTION
[0006] DHAA is a notoriously unstable chemical compound; in aqueous solution, particularly at neutral or basic pH and at warmer temperatures, it undergoes rapid hydrolysis to 2,3-diketogulonic acid (DKG) and irreversibly loses its vitamin C activity. Thus it is difficult and expensive to provide to consumers for convenient oral consumption. I have now found that DHAA can be provided conveniently and economically by creating it at the time of use, such that extended storage is not necessary. I have found that DHAA can be rapidly created by a simple method using AA (or some other form of reduced ascorbate, such as sodium ascorbate) as the substrate, using oxygen as a second substrate, and using an enzyme called Ascorbic Acid Oxidase that is found naturally in many plants, and is particularly abundant in zucchini fruits. Oxygen may be provided by stirring the mixture in air, or by bubbling air through the mixture.
Methods and the products produced by these methods are described here.
DESCRIPTION OF EMBODIMENTS
[0007] In a preferred embodiment, certain fresh, raw vegetables that contain the enzyme Ascorbic Acid Oxidase can be used to rapidly produce DHAA by oxidation of AA in a puree of the vegetable. For example, zucchini squash is known to contain extremely high levels of AAO. See Example 1.
[0008] In another embodiment, the peelings from the skin and fleshy middle layer (the epicarp and mesocarp) of zucchini fruit were used. It is known that the AAO enzyme is found at higher concentrations in the epicarp and outer mesocarp than in the endocarp and seeds of the zucchini fruit and other fruits and vegetables. By using the outer portions, a higher concentration of AAO can be obtained in a puree. See Example 2.
[0009] In another embodiment, AA was added in increments, or stages, to zucchini puree. It is known that AAO has an optimal pH range for activity, generally between about pH 4 and pH 9. It is also known that extreme pH values in solutions can prevent enzyme reactions from proceeding and even destroy the enzyme activity altogether. One way to take advantage of the powerful AAO enzyme activity of zucchini without killing the reaction with too much AA acidity is to add the AA in increments instead of all at once. As the AA is oxidized, the pH of the puree goes up since DHAA is not acidic. Then additional AA can be added. This process can be repeated many times, keeping the pH of the puree within the optimal pH range while accumulating very high concentrations of DHAA.
See Example 3.
[0010] Since DHAA is much less stable at neutral pH than at acidic pH, it is desirable to maintain the pH of a puree below about 7.0 during the oxidation process to avoid hydrolysis of the DHAA after it is produced. It is surprisingly found that a puree of zucchini is more acidic than pH 7.0 naturally, and it is also surprisingly discovered that as more AA is added, the pH of the final puree is more acidic. See Example 3.
[0011] In addition to AA, other forms of reduced vitamin C such as ascorbate ion can also be oxidized by AAO, including such salt forms as sodium ascorbate and calcium ascorbate, and chemical derivatives of AA such as ascorbyl phosphate and ascorbyl palmitate. All forms of reduced AA, including ascorbate and oxidizable derivates of AA may be employed in this process. I have found that concentrations of reduced vitamin C from as low as 0.1% w/w to as high as 20% w/w may be effectively oxidized according to the embodiments described here.
[0012] Acids, bases and buffers can be added to adjust the pH to desirable levels, before during or after the oxidation process.
[0013] Recovery of DHAA in the product is about 95%. See Example 3.
[0014] Product can be stored for at least 13 days frozen with minimal loss of DHAA. Therefore the product can be distributed in the frozen state. See Example 3.
[0015] The oxidized product can be further combined with polyol such as glycerin for longer stability, or flavoring, or texture adjustment.
[0016] Zucchini fruit, other vegetable matter containing AAO, or parts thereof can be frozen to preserve the natural AAO activity.
[0017] Dried or freeze-dried zucchini fruit or parts thereof can be used because enzyme activity is preserved on drying. AAO, and other enzymes, may be extracted from vegetables to create partially purified or highly purified extracts. These extracts may be dried or crystallized, or stabilized by other means to protect the enzyme activity. The dried vegetable matter or purified extracts can be combined with water and reduced vitamin C in a solution to create DHAA.
[0018] Agents that solubilize enzymes that are localized in the cell walls or cell membranes of plants can enhance the rate or reliability of the enzyme reaction or enhance the recovery of enzymes in extracts. Such agents include surfactants and detergents, chaotropes, and lytic enzymes. Representative agents include non-ionic detergents such as Triton-X, SDS, and lytic enzymes that specifically degrade the cell wall or cell membrane, including various proteases, pectinases, cellulases and hemicellulases.
[0019] Other agents can enhance enzyme activity or recovery and include agents to control ionic strength, osmotic strength, and the activity of nucleases and proteases.
[0020] Peroxidases and catalases in vegetables help stabilize AAO to prevent inactivation and exhaustion of the AAO during reaction. Using certain vegetables therefore provides the unexpected advantage of providing both AAO and peroxidase.
[0021] Numerous other vegetables contain AAO activity and/or catalase and/or peroxidase activity including Arabidopsis, Brassica, Cucumis, Cucurbita, Myrothecium, Nicotiana, Oryza, Sinapis, Titicum species, cabbage, squashes, pumpkins, peas, string beans, Lima beans, sweet corn, Swiss chard, carrots, parsnips, and spinach. Other vegetables can be used in this process to produce DHAA product. Combinations of different vegetables can be used to optimize the AAO/catalase/peroxidase ratios and to optimize the pH of a puree, or a solution, or a suspension of vegetable matter. Synthetic AAO enzyme may also be produced by methods known in the art, and may also be used instead of natural vegetable matter containing AAO.
[0022] A desirable product can be made by combining fruit(s) or vegetable(s) that is/are naturally high in AA content with fruit(s) or vegetable(s) that is/are naturally high in AAO content, to create a completely natural product containing a high content of DHAA.
[0023] A product can be made that is dried vegetable or vegetable parts plus AA or other form of reduced ascorbate, either mixed together or separately packaged, for rehydration and mixing with air to produce DHAA. This has the advantage of a stable enzyme, providing catalase and/or peroxidase, allowing proportions of enzyme vs. AA and time of reaction to be pre-determined, and assuring the oxidation reaction will work in the hands of the consumer.
[0024] A product can be in the form of a kit, including such additional components as a redox indicator, mixing vessel, instructions, gelatin, pH adjusters, mixing tools, etc.
[0025] The dried vegetable and AA, or the mixture of the two, can be distributed in pouches, unitized doses, tablets, capsules, or other convenient containers or easy to handle forms, including pre-measured amounts.
[0026] Gelatin capsules would provide gelatin for the reaction, which stabilizes AAO.
[0027] Copper can be added to a puree or solution containing AAO to enhance the activity and stability of the enzyme. Copper can be provided in the form of a soluble copper salt, or a solution containing dissolved copper, or by mixing the solution in a container made of copper. I have found that copper in the concentration of about 0.01 mg/dl up to about 20 mg/dl is effective for increasing the activity of the enzyme, and extending the period of time that the enzyme remains active before it is exhausted. Although copper ions alone are known in the art to increase the oxidation rate of AA in solution, this rate is much slower than the rate at which oxidation occurs in the presence of AAO. It is an unexpected discovery that the AAO enzyme activity is greatly increased, i.e. to a much higher rate than would be expected due to the copper activity alone, by the presence of copper ions in the concentrations described. It is an unexpected and surprising discovery that the enzyme remains active for longer periods of time when copper ions are added. This effect may be attributable to providing additional copper ions that are available to restore the copper ions found naturally in the AAO enzyme, as it has been reported that copper ions are exchanged between the enzyme and the solution during the oxidation process. The applicant does not wish to be held to this explanation, however, as other explanations are possible.
[0028] AA concentration in solution is commonly measured as the reducing activity of the solution using starch-iodine titration methods that are well-known in the art. Modification of the starch-iodine titration method can be used to detect AA in a vegetable/AA puree and therefore provide a process and a product for determining if and when AA has been converted to DHAA. A product or reagent for this process can be described as a redox indicator reagent.
[0029] A redox reagent can be made by combining iodine, iodide, and starch in solution. Such redox reagent can be optimized in concentration, or utilized in various amounts, to indicate various concentrations of AA.
[0030] Starch-iodine redox reagent can be dried on paper or immobilized by other methods to provide a convenient test such as a paper test strip or pad.
[0031] A redox reagent utilizing a different chemical or chemicals known to be indicators of reduction-oxidation potential can be used.
[0032] Progress of oxidation of AA to DHAA may be monitored by pH measurements.
[0033] A business method can involve the production of “vegetable smoothies” containing DHAA in retail outlets, or licensing or franchise.
[0034] A business method can involve the licensing of the rights or directions to produce DHAA.
[0035] An apparatus optimized to puree the vegetable, or enhance air or oxygen incorporation, or otherwise improve upon available apparatus can be made.
[0036] An oxygen-generating chemical additive, or air pump, or enriched oxygen gas can be incorporated.
[0037] Flavorings or colors can be added to enhance the flavor or appearance of the product. In particular, flavorings selected from the group not including sugars that are absorbed by the same GLUT transporters that transport DHAA are preferred, because sugars that are transported by the same transporters may competitively inhibit the transport of DHAA.
EXAMPLES
Example 1
[0038] Two cups of diced zucchini fruit were placed in a 2-quart blender with about 1⁄2 cup water and pureed for about 1 minute. Four commercially available vitamin C tablets containing 1000 mg AA each (Kirkland brand, Item 98268, Lot T00007 from Costco) were dissolved in 1⁄4 cup hot water and added to the puree. Blender was capped and turned on to mix and the puree was tested periodically using a starch-iodine redox indicator for the presence of AA reducing activity.
At about one minute, the redox indicator showed the presence of AA reducing activity. Within 10 minutes, the redox indicator showed that no more AA reducing activity was present in the puree, demonstrating that all of the AA in the puree had been oxidized to DHAA by oxygen that had been mixed into the puree from the air inside the blender, catalyzed by the AAO activity of the enzyme in the zucchini.
Example 2
[0039] Four zucchini fruits about 6-8 inches long were purchased at a local grocery store. The shelf labeling indicated the fruits were a product of Mexico, as might be expected in Utah during the month of November when this experiment was conducted. Thus the fruit was not locally-grown and probably older (stored longer since picked) than known fresh-picked fruit. It is known that the AAO activity of zucchini fruit decreases during storage after being picked. The epicarp and outer portions of the mesocarp were peeled from the fruits, to the extent that approximately one-half of the weight of each fruit was included in the peelings. 300 grams of peelings were added to a blender with 100 grams purified water and pureed. 20 grams of the puree was removed and reserved for a “blank”. To the remaining puree (380 grams) was added 1.4 grams AA (as pure crystals approximately US mesh size 20-40) and the puree was mixed in the blender about 1 minute. The pH of the puree was measured and found to be 5.2, and a redox test indicated AA reducing activity in the puree. The puree was allowed to stand with periodic brief mixing for 35 minutes. At this point, the pH was 6.5 and the redox test showed that all AA was oxidized. A 20 gram portion was removed for a “test.” The blank and test solutions were centrifuged to remove the pulp so that pulp-free solutions could be spectrophotometrically analyzed. 25 uL of each of these solutions were diluted in 10 mL of 0.15 M phosphoric acid diluent, and the absorbance of each was determined using a UV spectrometer at 262 nm wavelength blanked against diluent. 2 mL of each dilution were combined with 2 mL of a TCEP reagent, incubated one hour, and then the absorbance at 262 nm of these solutions were determined as above (TCEP reagent reduces DHAA in the solution to AA; absorbance measurements at wavelengths where AA strongly absorbs, before and after treatment with TCEP, is a method known to practitioners in the art to quantify DHAA concentration by the differential absorption principle). The following absorption values were obtained (TCEP values are corrected for the X2 dilution):
Sample Abs 262 (mAU) Abs post TCEP Abs Difference
Blank 0.060 0.068 0.008
Test 0.060 0.268 0.208
[0040] The Abs difference demonstrates that substantial amounts of DHAA are present in the “Test” puree as compared to the “Blank” puree.
Example 3
[0041] One whole zucchini fruit weighing 235 grams was pureed in 120 mL water in a blender. The pH of the initial zucchini puree was 6.5. At time 0 minutes, 1.0 gram crystalline AA was added. After mixing 30 seconds, the pH was 5.0. At the times indicated in the table below, pH was recorded, iodine indicator redox result was recorded, and/or additional AA in the amounts indicated were added after testing the pH and redox status. The zucchini puree was continuously mixed in the blender during the entire time, and a cap in the top of the blender was left open to allow fresh air to be drawn into the vortex of the puree in the blender. The redox test results are reported + or −, ‘+’ indicating that AA reducing activity was detected, and ‘−’ indicating that AA reducing activity was not detected.
Time (min.) pH Redox (+ or −) AA added (g)
0 6.5 − 1.0
5 5.0 + 0.0
10 5.0 + 0.0
15 5.3 + 0.0
20 6.6 − 0.5
25 6.4 − 0.5
29 6.3 − 0.5
33 5.9 − 0.5
36 5.9 − 0.5
40 5.6 − 0.5
45 5.4 − 0.5
48 5.2 − 0.5
52 5.0 − 0.5
56 5.0 − 0.5
59 4.8 − 0.5
62 4.7 − 0.5
67 4.5 − 0.5
71 4.4 − 0.5
77 4.3 − 0.5
89 4.5 − 0.0
Total AA added = 8.5 grams.
DHAA Max. Expected Concentration = 8.5 g/355 g solution = 2.4% w/w.
[0042] The product was split into three equal parts. Part 1 was kept in a closed container at room temperature. Part 2 was kept in a closed container at standard refrigerator temperature of 4 degrees C. Part 3 was kept in a closed container at common freezer temperature of minus 20 degrees C. Part 1 was tested immediately for DHAA concentration by the TCEP method previously discussed, and then after overnight storage (approx. 12 hours); Part 2 was tested after overnight storage (approx. 12 hours), and then after 13 days; Part 3 was tested after 13 days. Results are shown in the table below. Recovery column is the actual concentration divided by the maximum expected DHAA concentration of 2.4%, expressed as percent.
DHAA
Sample Storage (hours) Concentration Recovery %
Part 1 (Immediate) 0 2.27% 95%
Part 1 (Room Temp) 12 1.68% 70%
Part 2 (Refrig.) 12 2.14% 89%
Part 2 (Refrig.) 312 (13 d) 1.27% 53%
Part 3 (Freezer) 312 (13 d) 2.10% 89%
STABLE COMPOSITIONS OF DEHYDROASCORBIC ACID
The invention relates to stable liquid compositions containing the oxidized form of vitamin C known as dehydroascorbic acid (DHAA). The compositions comprise DHAA and a pharmacologically acceptable liquid organic polyol solvent. The polyol solvent comprises about 50% or greater of the total weight of the composition. The compositions are useful as dietary supplements, skin-enhancers, concentrates, or research solutions.
BACKGROUND
[0002] 1. Field of Invention
[0003] This invention relates to compositions of matter used as sources of vitamin C in dietary supplementation, skin care products, therapy, research, and manufacturing. More specifically, the invention relates to stable liquid compositions containing the oxidized form of vitamin C known as dehydroascorbic acid.
[0004] 2. Prior Art
[0005] Ever since the elucidation of the chemical structure of vitamin C in the mid-1930's it has been known that vitamin C occurs naturally as two different compounds, namely, ascorbic acid (AA) and an oxidized form of AA called dehydroascorbic acid (DHAA). It also is known that AA and DHAA are unstable compounds. In aqueous solutions, some factors which affect the rate of their destruction include the pH of the solution, and exposure to various metal ions, heat, light and air. It also is known that DHAA is considerably less stable than AA when subjected to comparable conditions. ‘Deutsch J C. Dehydroascorbic acid. Review Journal of Chromatography A, 881 (2000) 299-307’ (Deutsch), incorporated here by reference, states en-equivocally “DHA is more reactive and unstable in solution than AA.” Therefore, as a supplement to the diet, or as an ingredient of a topically applied product such as a skin lotion, AA has been the preferred chemical form of vitamin C because of its greater stability. In fact, we do not know of any commercially available dietary or topically applied product wherein DHAA specifically has been utilized as a substantial source of vitamin C.
[0006] Also known is that solid AA is far more easily dissolved in water than is solid DHAA, as noted in ‘Pecherer B J. The Preparation of Dehydro-L-ascorbic Acid and its Methanol Complex. Am Chem Soc 73 (1951) 3827-3830’ (Pecherer) and ‘Koliou E K and Ioannou P V. Preparation of dehydro-L-ascorbic acid dimer by air oxidation of L-ascorbic acid in the presence of catalytic amounts of copper(II) acetate and pyridine. Carbohydrate Research 340 (2005) 315-318’ (Koliou) which are incorporated here by reference. To prepare aqueous solutions of DHAA from the solid form requires prolonged mixing at temperatures well above 37 degrees centigrade. Thus solutions of DHAA are much more difficult to manufacture than solutions of AA. Also, since the conditions to solubilize it efficiently do not exist in the gut of human or other animals, substantial doubt exists about whether the dry, solid form of DHAA can be absorbed when ingested. These are also reasons why DHAA has not been utilized as the source of vitamin C for dietary supplements or topical products.
[0007] Around the same time as the chemical structures of AA and DHAA were elucidated in the mid- 1930's, the antiscorbutic properties (ability to prevent the disease called scurvy) of both compounds were recognized and generally accepted as being equal or nearly so. The oxidation of AA to DHAA was shown to be reversible both in vitro and in biological systems, so the equivalence of the two compounds could easily be attributed to simple interconversion within an organism. Although a few early investigators did note some peculiar differences in the biological utilization of these two compounds, at least as essential dietary ingredients for humans and certain other species, AA and DHAA were generally considered bioequivalent. The dietary supplement and skin care product industries developed their products using AA (and various more stable derivatives of AA) because of the stability and solubility issues with DHAA, and DHAA has essentially been ignored and forgotten in these industries.
[0008] Since the mid-1930's, the volume of research in vitamin C has been enormous, and it is possible that no single subject in the field of biology has been the focus of more research and more scientific journal articles than vitamin C. And since about the mid-1990's, many new discoveries about DHAA have been made. Among these discoveries, those of particular pertinence to the present invention include those which demonstrate that, although the two compounds are equivalent in their antiscorbutic properties, AA and DHAA are not “bioequivalent” in any broad definition of the word. Specifically it is known today that AA and DHAA are absorbed by different mechanisms in the gut; that they accumulate differently in the various tissues of an animal when ingested; that they are absorbed into living cells by completely different mechanisms utilizing different receptors on the cell surface; that the cells of certain important tissues of the human body (e.g., brain) have a very high concentration of vitamin C but completely lack cell surface receptors for AA; that DHAA is absorbed into cells by the same receptors as glucose, which are present on every cell in the human body; that in human skin cells, DHAA is absorbed up to 5 times faster and to levels 2 times higher than is AA; that DHAA is almost instantly converted into AA once it has been absorbed into a cell; that both AA and DHAA have antiviral effects in vitro against viruses that cause disease in humans such as HSV-1 (herpes simplex virus type 1 that causes oral herpes and can cause genital herpes), influenza virus, and poliovirus; and that DHAA has much stronger antiviral effects than does AA. Literature that supports these statements, and is incorporated here by reference, includes ‘Savini et al. Dehydroascorbic acid uptake in a human keratinocyte cell line (HaCaT) is glutathione-independent. Biochem J 345 (2000) 665-672’ (Savini) and ‘Furuya et al. Antiviral effects of ascorbic and dehydroascorbic acids in vitro. Int J Mol Med 22 (2008) 541-545’ (Furuya).
[0009] Thus it can be seen that a solution of DHAA for oral ingestion or topical application, while being a source of vitamin C much like numerous other available products that contain AA, also can provide specific benefits and uses unavailable in any other product on the market today. What is needed is a stable liquid solution of DHAA in an orally and topically acceptable medium.
[0010] U.S. Pat. No. 5,140,043 (Darr) discloses topical compositions of ascorbic acid (or a reducing analog of ascorbic acid) in a water-(glycol or polyol) carrier, wherein the ratio of water to glycol/polyol carrier is high (e.g., at least 1:1). These solutions of Darr do not contain DHAA, and Darr is silent as to the stability of the non-reducing compound DHAA in this carrier. We have found that DHAA is not stable in polyol solutions containing such high concentrations of water, which points out that no assumptions about the chemical and physical behavior of DHAA in polyol solutions should be drawn from the behavior of AA in those solutions. While AA and DHAA share certain biological functions, they are two different molecules in regard to their physical and chemical behavior, including stability.
[0011] U.S. Pat. No. 6,197,813 (Hegenauer) discloses stable vitamin C compositions of mineral ascorbates in liquid organic polyol solvents having pH values of about 5 to 7, but is silent as to the stability of the non-mineral DHAA in those solvents. These compositions of Hegenaur do not contain DHAA. In fact, these compositions do not even contain a naturally-occurring form of vitamin C, and therefore if these compositions were applied to the skin, vitamin C would not be expected to be absorbed by either the ascorbic acid receptors or the glucose receptors of skin cells.
[0012] US Patent Application 2009/0016974 A1 (Pruche et al) discloses DHAA-containing compositions formed “in situ” from ascorbic acid via chemical oxidation and/or via enzymatic oxidation, and a two-component agent thereof These compositions attempt to overcome the instability of DHAA by preparing it fresh as needed, but they require handling and mixing steps of the two-component agent. The two components must be stored separately. Chemical oxidizers are harsh and can be dangerous, and enzymes are unstable, thus these compositions are problematic in regard to safety and reliability. Since the two components are intended to be combined by the end user, the temperature of the reaction and other conditions necessary for reliable oxidation processes are beyond the control of the manufacturer. Without some separate indicator, the final consumer cannot be assured that the solution prepared by the two-component system actually contains DHAA, because the oxidation of AA to DHAA is not visually or otherwise simply detected. These compositions do not contain DHAA pre-prepared in a stable solution, and Pruche et al is silent as to the stability of DHAA in the disclosed compositions.
Objects and Advantages
[0013] Several objects and advantages of the present invention are:
a. To provide compositions containing DHAA in a stable form.
b. To provide stable DHAA-containing compositions for topical application to the skin of a human or animal as a source of highly absorbable vitamin C.
c. To provide compositions for topical application that are pharmacologically acceptable and pleasant to use.
d. To provide compositions for topical application that can be applied alone, or mixed with water to provide greater humidifying effect, or mixed with another skin care product to enhance the vitamin C content of that product.
e. To provide compositions containing DHAA for topical application that can also solubilize other skin-enhancing substances that are insoluble in water, such as vitamin E.
f. To provide stable DHAA-containing compositions for dietary supplementation of a human or animal as a source of highly absorbable vitamin C.
g. To provide compositions for dietary supplementation that are pharmacologically acceptable and pleasant to use.
h. To provide compositions for dietary supplementation that can be taken orally alone, or mixed with water or some other liquid, or applied to solid food.
i. To provide stable DHAA-containing concentrates for manufacturing of other products.
j. To provide stable DHAA-containing compositions that can be conveniently used in research, for example in chemical studies, or in microbial culture or tissue culture.
k. To provide stable DHAA-containing compositions that do not require the addition of chemical stabilizers or preservatives.
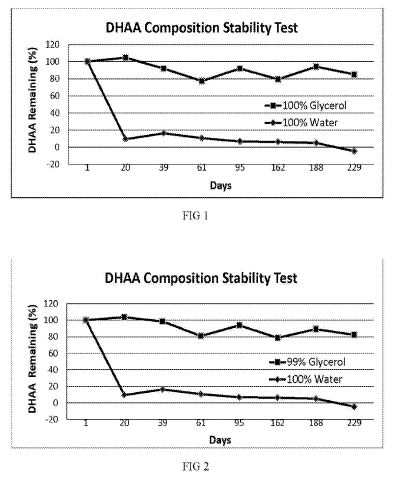
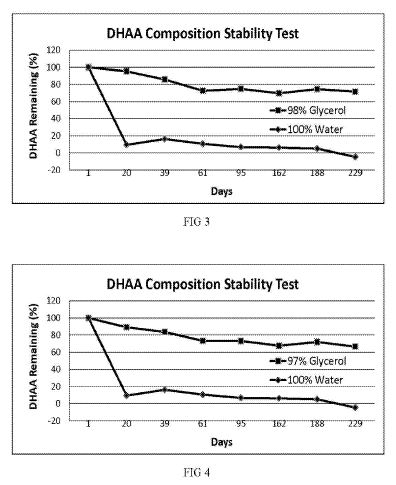
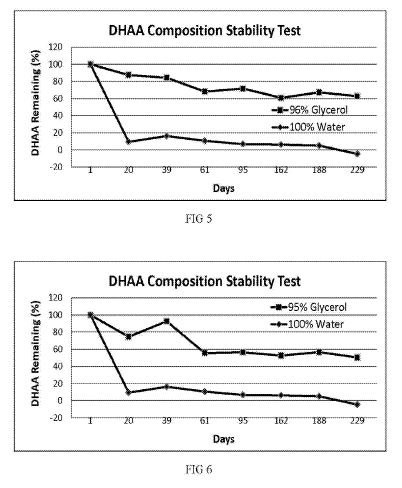
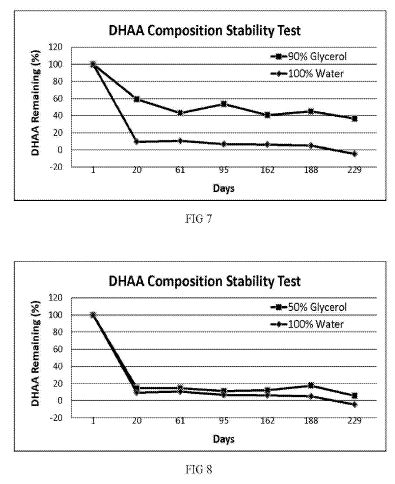
DRAWING FIGURES
[0025] FIGS. 1 to 8 show the DHAA stability of the various compositions described in Example 1 as compared with DHAA prepared similarly in water.
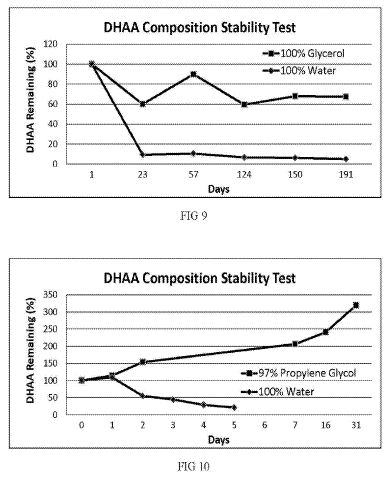
[0026] FIG. 9 shows the DHAA stability of the composition described in Example 2 as compared with DHAA prepared in water.
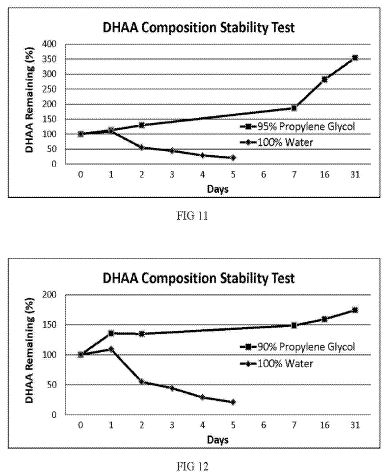
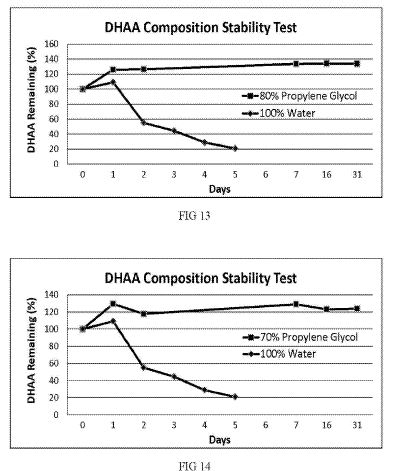
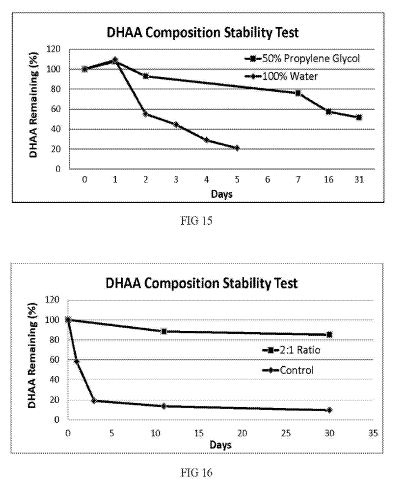
[0027] FIGS. 10 to 15 show the DHAA stability of the compositions described in Example 3 as compared with DHAA prepared similarly in water.
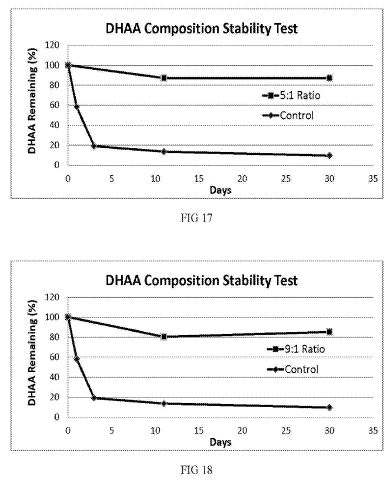
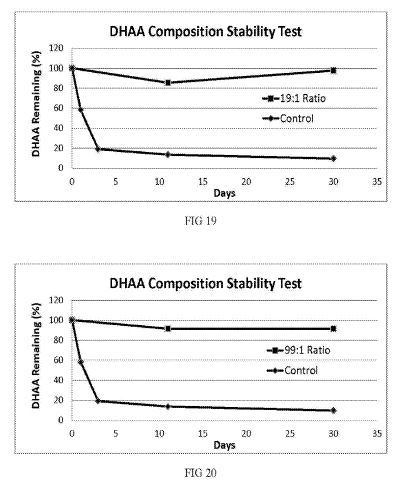
[0028] FIGS. 16 to 20 show the DHAA stability of the solutions described in Example 4.
[0029] FIG. 21 shows the absorption of AA and DHAA into skin as described in Example 5.
DESCRIPTION
[0030] We have discovered that DHAA is stable in solutions of pure polyol solvents and in solutions wherein the polyol content is greater than about 50 percent. By “stable” is meant that DHAA in these solutions deteriorates very slowly over a sufficient period of time that it can be stored and sold as a dietary supplement or as a skin care product, or as a concentrate for preparing or manufacturing them, with a reasonable shelf life.
[0031] In one embodiment, a DHAA composition is provided wherein the composition comprises 50% or more polyol by weight and a ratio of DHAA to AA of from greater than 1:100, 1:50, 1:10, 1:5, 3:10, 1:2, 1:1, 2:1, 10:3, 5:1, 10:1, 50:1, or 100:1.
[0032] In one embodiment, a DHAA composition is provided wherein the composition comprises 50% or more polyol by weight and greater than 0.05%, 0.25%, 0.5%, 0.83%, 1.7, or 2.5% DHAA.
[0033] In one embodiment, a DHAA composition is provided wherein the composition comprises 50% or more polyol by weight and about 0.85% to 15% DHAA.
[0034] In one embodiment, a method of treating a disease or condition is provided comprising identifying an individual in need of treatment and administering to said individual a DHAA composition comprising 50% or more by weight of a polyol. In one aspect, the DHAA composition comprises a pharmaceutically acceptable carrier. In one aspect, the composition is suitable for oral administration. In one aspect, the composition is suitable for intravenous administration. In one aspect, the composition is suitable for intraperitoneal administration. In one aspect, the composition is suitable for topical administration.
[0035] In some embodiments, the method of treating a disease or condition comprises identifying an individual having a disease or condition that may be treated by DHAA, AA, or a combination thereof.
[0036] In some embodiments, the method of treating a disease or condition further comprises administration of a second agent. In some aspects, the second agent is an anti-cancer agent, an antiviral agent, or an agent used for treating a neurodegenerative disease or condition.
[0037] The solutions are made by oxidizing ascorbic acid that is first dissolved in a pure polyol solvent, or in water, or in some mixture of these liquids. The polyol concentration may be adjusted to about 50% or greater prior to oxidizing the AA or afterwards.
[0038] The solutions can also be made by oxidizing AA that is dissolved in an alcohol (e.g., ethanol), and then combining the DHAA-containing alcohol with a polyol solvent. If it is desired that the final solution does not contain alcohol, the alcohol can be removed by evaporating the alcohol from the polyol solvent solution using heat or vacuum, or both.
[0039] The solutions can also be made by dissolving solid DHAA in a pure polyol solvent, or in water, or in some mixture of these liquids. The polyol concentration may be adjusted to about 50% or greater prior to dissolving the DHAA or afterwards.
[0040] The organic polyol solvents are chosen for pharmaceutical and dietary acceptability, their ability to solubilize the AA and DHAA component, water content, and effect on the stability of the DHAA component. At present we prefer to employ commercially available glycerol which generally contains 5% or less water. In general, we prefer to minimize the water content of the solvent(s), consistent with economic and functional considerations. Other polyols which can be employed include propylene glycol, hexylene glycol, butylene glycol and the almost infinite molecular weight range of polyethylene glycols, as well as so-called sugar alcohols, e.g., sorbitol and xylitol, and mixtures thereof with other polyols.
[0041] These solutions can be prepared entirely with one polyol solvent, e.g., glycerol, or mixtures of polyol solvents. The final choice of solvent will depend on economics and other relevant factors.
[0042] Methods we have successfully applied for oxidizing the ascorbic acid include the use of halogen or ozone or oxygen/activated charcoal or Fenton's Reagent or ascorbic acid oxidase enzyme. All of these methods are known in the art, as are other methods; the previously cited references Pecherer and Koliou show typical applications of various methods for example. The method by which the oxidation is accomplished is not the determinant factor of the long term stability of the DHAA in the solution, and other methods of oxidation are within the scope of the invention.
[0043] AA concentration in solution is commonly measured as the reducing activity of the solution using starch-iodine titration methods that are well-known in the art. AA is also measured by ultra-violet spectrophotometry using a wavelength at which AA absorbs strongly and DHAA does not, typically about 265 nm.
This method is also well known in the art. DHAA in solution can be converted into AA by reducing agents such as dithiothreitol (DTT) or tris(2-carboxyethyl)phosphine (TCEP), and its concentration is commonly measured spectrophotometrically as the difference in absorbance of a solution subjected to reduction by DTT or TCEP versus a similar solution that is not subjected to a reducing agent. These methods are also well-known in the art, but see Deutsch for examples. In the description, claims, and the following examples, DHAA in the compositions of the invention is the vitamin C that can be measured by the difference in absorbance at 262 nm using TCEP reducing agent.
[0044] The following embodiments are exemplary of the invention:
Example 1
[0045] In a preferred embodiment of the invention, AA dissolved in glycerol and/or water is oxidized using ozone to produce DHAA solutions. Water-based solutions and glycerol-based solutions may be combined to yield stable DHAA compositions having the desired polyol concentration.
[0046] A 15% AA solution in water was prepared by adding 15 grams AA per 100 mL purified water with stirring. A 15% solution of AA in glycerol was prepared by adding 15 grams AA per 100 mL pure USP glycerol and stirring with heat. A corona-discharge type ozone generator with feed-gas of pure oxygen was used to supply an oxidizing gas containing about 5% ozone, and each of the 15% AA solutions was subjected to oxidizing conditions by bubbling the oxidizing gas through the solution using a glass diffuser. The progress of AA oxidation in each solution was monitored by the disappearance of reducing activity as measured by starch-iodine titration. Each solution was subjected to the oxidizing conditions until all (>99%) of the original reducing activity had disappeared. The solution made with pure glycerol was labeled “100% Glycerol,” and the solution made with purified water was labeled “100% Water.” Portions of these two solutions were combined to produce solutions of various glycerol concentrations by weight, specifically “99% Glycerol,” “98% Glycerol,” “97% Glycerol,” “96% Glycerol,” “95% Glycerol”, “90% Glycerol,” and “50% Glycerol.” For example, 99 parts by weight of “100% Glycerol” was combined with 1 part by weight “100% Water” to produce the “99% Glycerol” solution.
[0047] Aliquots of each of the solutions prepared above were placed in translucent, screw-capped polyethylene vials and were stored at room temperature. No attempt was made to further protect the vials from ambient indoor light, and each vial contained a headspace of normal air. Each vial was periodically opened to remove a sample for stability testing over the next 229 days. The concentration of DHAA in each sample was measured by spectrometry on each testing day.
The initial DHAA concentration of each solution on Day 1 was recorded and assigned a value of 100%, and the concentration on each subsequent stability test day was calculated as the percent remaining of the initial concentration.
[0048] FIGS. 1 through 8 show the results of stability testing of the various glycerol-containing solutions; each graph also shows the result of the “100% Water” solution for comparison. It can be seen that DHAA decomposes rapidly in water. By the time the water solution was tested at 20 days, less than 10 percent of the initial amount of DHAA remained. By contrast, DHAA is preserved very well in solutions containing high concentrations of glycerol. In pure glycerol for example, greater than 80% of the initial DHAA concentration remains even after approximately 8 months of storage at room temperature. As the glycerol concentration is reduced, stability is reduced, until only minor improvement is gained at 50% glycerol concentration.
Example 2
[0049] In another embodiment, a stable DHAA composition is produced by oxidation of AA dissolved in glycerol using exposure to activated charcoal and oxygen as the oxidation method.
[0050] A solution of AA in pure USP glycerol was subjected to oxidizing conditions by suspending activated charcoal in the solution and then bubbling pure oxygen through the solution. Oxidation of AA during this process was monitored by starch-iodine titration. After the desired amount of AA had been oxidized, the activated charcoal was removed from the solution by centrifugation and filtration. This solution was labeled “100% Glycerol.” A portion of the solution was then placed in a translucent, screw-capped polyethylene vial and was stored at room temperature. No attempt was made to further protect the vial from ambient indoor light, and the vial contained a headspace of normal air. The vial was periodically opened to remove a sample for stability testing over the next 191 days. The concentration of DHAA in the sample was measured by spectrometry on each testing day. The initial DHAA concentration of the solution on Day 1 was recorded and assigned a value of 100%, and the concentration on each subsequent stability test day was calculated as the percent remaining of the initial concentration.
[0051] FIG. 9 shows the results of the stability testing of this solution, and for comparison also shows the stability of a DHAA solution prepared in purified water (labeled “100% Water”). It can be seen that DHAA in glycerol produced by an alternative oxidation method shows excellent long-term stability.
Example 3
[0052] In another embodiment, stable DHAA compositions are produced by oxidizing AA dissolved in water using Fenton's Reagent as the oxidizing method, and then combining the water solution with propylene glycol such that the final concentration of polyol is 50% or greater.
[0053] AA was dissolved in purified water to give a highly concentrated solution, and then sufficient 30% hydrogen peroxide was added to oxidize about half of the AA. Iron to catalyze the reaction was provided by addition of ferrous sulfate. Oxidation of the AA was monitored by spectrometry until the expected amount of AA had been oxidized. This solution was labeled “100% Water.” Portions of this solution were combined with portions of pure, USP grade propylene glycol to produce solutions of “97% Propylene Glycol,” “95% Propylene Glycol,” “90% Propylene Glycol,” “80% Propylene Glycol,” “70% Propylene Glycol,” and “50% Propylene Glycol.” For example, 3 parts by volume of the “100% Water” solution were combined with 97 parts by volume propylene glycol to yield the “97% Propylene Glycol” solution.
[0054] Aliquots of each of the solutions prepared above were placed in translucent, screw-capped polyethylene vials and were stored at room temperature. No attempt was made to further protect the vials from ambient indoor light, and each vial contained a headspace of normal air. Each vial was periodically opened to remove a sample for stability testing over the next 31 days. The concentration of DHAA in each sample was measured by spectrometry on each testing day.
The initial DHAA concentration of each solution was recorded and assigned a value of 100% (Day 0), and the concentration on each subsequent stability test day was calculated as the percent remaining of the initial concentration.
[0055] FIGS. 10 through 15 show the results of stability testing of the various propylene glycol- containing solutions; each graph also shows the result of the “100% Water” solution for comparison. It can be seen that DHAA decomposes rapidly in water; after only 5 days, less than 20 percent of the initial amount of DHAA remains. By contrast, DHAA is preserved very well in solutions containing high concentrations of propylene glycol. In fact, the DHAA concentration in many of these solutions actually increased significantly over time, a remarkable and unexpected discovery. We believe this phenomenon can be explained this way: residual AA continues to oxidize while the DHAA is stabilized and therefore accumulates in the solution. The spectrophotometric measurements support this explanation, but we do not wish to be bound by this explanation.
Example 3
[0056] demonstrates that stable DHAA compositions may be prepared using a third alternative oxidation method as compared with the first two examples, and also demonstrates that an alternative polyol solvent can be used.
Example 4
[0057] In another embodiment, stable DHAA compositions containing various ratios of AA:DHAA are demonstrated.
[0058] A first solution was prepared containing AA and DHAA in 100% glycerin, wherein the ratio of AA:DHAA was about 1:1, and the actual concentrations of AA and DHAA was about 2.5% by volume respectively. Therefore the total vitamin C concentration in the first solution was about 5%. A second solution was prepared containing only AA in 100% glycerin, and wherein the AA concentration was about 5% by volume. Various proportions of the first solution and the second solution were combined to produce other solutions that each contained a total vitamin C concentration of about 5%, but wherein the ratio of AA:DHAA varied between about 1:1 and about 99:1. More specifically, solutions were prepared that contained AA:DHAA ratios of about 2;1, 5:1, 9:1, 19:1, and 99:1.
[0059] For comparison, a solution was prepared containing AA and DHAA in 100% water, wherein the ratio of AA:DHAA was about 1:1, and the total vitamin C content was about 5%. This solution was designated “Control.”
[0060] Aliquots of each of the solutions prepared above were placed in transparent, screw-capped glass vials and were stored at room temperature. No attempt was made to further protect the vials from ambient indoor light, and each vial contained a headspace of normal air. Each vial was periodically opened to remove a sample for stability testing over the next 30 days. The concentration of DHAA in each sample was measured by spectrometry on each testing day. The initial DHAA concentration of each solution was recorded and assigned a value of 100% (Day 0), and the concentration on each subsequent stability test day was calculated as the percent remaining of the initial concentration.
[0061] FIGS. 16-20 show the results of stability testing of the various solutions; each graph also shows the result of the “Control” solution for comparison.
It can be seen that DHAA decomposes rapidly in water when the initial ratio of AA:DHAA is about 1:1; after only 3 days, less than 20 percent of the initial amount of DHAA remains. By contrast, DHAA is preserved very well in polyol solutions containing AA:DHAA ratios of between 2:1 and 99:1
Example 5
[0062] A solution containing both AA and DHAA dissolved in pure glycerol was prepared. Concentrations of AA and DHAA were about 2.5% respectively. This solution was applied topically to the skin of human volunteers to compare the absorption rate of AA versus DHAA. To assess permeation into the stratum corneum, the solution was diluted 1:1 with water and applied at a rate of 1.4 mg/cm<2 >to delineated skin surfaces and allowed 0, 2 or 4 hours for absorption. Each skin surface was then washed with deionized water, and the skin washings were collected and measured for AA and DHAA content. The amount absorbed at 2 and 4 hours was determined by subtraction from the amount present in the 0 hour washings.
[0063] FIG. 21 shows the absorption of AA and DHAA into skin. Data points are the mean +/− SD of triplicate analyses on 4 subjects. The 2 and 4 hour values are the difference as percentage from the 0 hour (baseline) values, determined by analysis of skin washings. It can be seem that after 4 hours DHAA had absorbed into the skin at a rate about 12 times greater than AA, and that the total vitamin C content of the skin was increased at a much more rapid rate than applying AA alone. (Asterisks on FIG. 21 indicate the following: * Statistically significant at P<0.05. ** Statistically significant at P<0.01).
Example 6
[0064] A solution containing both AA and DHAA dissolved in pure glycerol was prepared. Concentrations of AA and DHAA were about 2.5% respectively. One part solution was diluted with 9 parts water to give a working solution. The AA and DHAA concentrations of this working solution were measured and recorded. About 20 grams of this solution was taken into the mouth by a human volunteer. Over the course of 5 minutes, the volunteer intermittently rinsed the oral cavity with the working solution by swiahing the solution about in the mouth, or gargled with the solution to rinse the tissues of the throat, being careful to avoid swallowing any of the working solution. At the end of 5 minutes, the volunteer expectorated the fluid, which was collected and weighed. The AA and DHAA concentrations of the expectorated fluid were measured and recorded. The amount of AA and DHAA absorbed into the tissues of the mouth and throat was determined by subtraction from the concentrations determined on the solution before application to the mouth. Results were corrected for the dilution effect of accumulated saliva according to the difference in weight of fluid taken into the mouth as compared to the weight of the expectorated fluid. The results showed that approximately 13.2% of the total AA was absorbed, and that approximately 14.8% of the DHAA was absorbed.
Conclusion, Ramifications, and Scope
[0065] While the above description contains many specificities, these should not be construed as limitations on the scope of the invention, but rather as exemplification of preferred embodiments. The compositions can be prepared using various methods and ingredients as mentioned, and their equivalents. Polyol solvents are known to be antimicrobial in high concentrations and therefore the compositions of the invention generally do not require preservatives. Polyol solvents are also capable of dissolving substances that are not soluble in water, so are capable of solubilizing not only AA and DHAA but additional dietary or skin-enhancing ingredients such as vitamin E. Many polyol solvents are excellent skin-enhancing substances in their own right, such as glycerol which is commonly utilized in skin care products as a humectant. Many polyol solvents are not only safe for ingestion, but in fact have a pleasant, sweet flavor. Thus the compositions have favorable properties that are synergistic with their use as dietary supplements, skin-enhancers, concentrates, or research solutions.
STABLE COMPOSITIONS OF DEHYDROASCORBIC ACID
Stable liquid compositions containing the oxidized form of vitamin C known as dehydroascorbic acid are provided. The compositions comprise dehydroascorbic acid and a pharmacologically acceptable liquid organic polyol solvent for said dehydroascorbic acid, wherein said polyol solvent comprises about 50% or greater of the total weight of said composition. The compositions are useful as dietary supplements, skin-enhancers, concentrates, or research solutions.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1080727/
Plant Physiol. 1991 May; 96(1): 159–165.
PMCID: PMC1080727
Liang-Shiou Lin and Joseph E. Varner
Abstract
The expression of ascorbic acid oxidase was studied in zucchini squash (Cucurbita pepo L.), one of the most abundant natural sources of the enzyme. In the developing fruit, specific activity of ascorbic acid oxidase was highest between 4 and 6 days after anthesis. Protein and mRNA levels followed the same trend as enzyme activity. Highest growth rate of the fruit occurred before 6 days after anthesis. Within a given fruit, ascorbic acid oxidase activity and mRNA level were highest in the epidermis, and lowest in the central placental region. In leaf tissue, ascorbic acid oxidase activity was higher in young leaves, and very low in old leaves. Within a given leaf, enzyme activity was highest in the fast-growing region (approximately the lower third of the blade), and lowest in the slow-growing region (near leaf apex). High expression of ascorbic acid oxidase at a stage when rapid growth is occurring (in both fruits and leaves), and localization of the enzyme in the fruit epidermis, where cells are under greatest tension during rapid growth in girth, suggest that ascorbic
acid oxidase might be involved in reorganization of the cell wall to allow for expansion. Based on the known chemistry of dehydroascorbic acid, the end product of the ascorbic acid oxidase-catalyzed reaction, we have proposed several hypotheses to explain how dehydroascorbic acid might cause cell wall “loosening.”
http://www.jbc.org/content/248/19/6596.full.pdf
Further Studies on the Purification of the Enzyme
by Men Hui Lee
Purification of ascorbate oxidase from green zucchini squash. (Cucurbita pepo meduttosa). The new purification method achieves a more than 200-fold purification...
https://chem.libretexts.org/LibreTexts/University_of_California_Davis/UCD_Chem_124A%3A_Berben/Ascorbate_Oxidase
Ascorbate oxidase is a multi-copper enzyme that catalyzes the oxidation of ascorbic acid to dehydroascorbic acid. This copper containing blue enzyme is found in cucurbitaceous plants such as pumpkin, cucumber, and melon. It can eliminate ascorbic acid, which has high reducing power in clinical analyses, and detect levels of ascorbic acid. The biological function of ascorbate oxidase is still not clear. One suggestion is that the enzyme participates in a redox system involving ascorbic acids. It may be involved in the reorganization of the cell wall. In pumpkins, ascorbate oxidase expression increased rapidly during growth of callus, development of fruits, and elongation of seedlings. Ascorbate oxidase is present in young and growing tissues of tobacco. It is induced by phytohormone auxin which suggests that it is involved in cell growth...
Method for increasing the concentration of ascorbic acid in brain tissues of a subject
Inventor(s): AGUS DAVID / VERA JUAN / GOLDE DAVID
Applicant(s): SLOAN KETTERING INST CANCER
This invention provides a method for increasing the ascorbic acid concentration in brain tissues of a subject which comprises administering to the subject an amount of dehydroascorbic acid effective to increase the concentration of ascorbic acid in brain tissues. This invention also provides that the dehydroascorbic acid enters the tissues through the facilitative glucose transporter.